Diagnosis
The two main types of lung cancer are:
- small cell lung cancer (SCLC)
- non-small cell lung cancer (NSCLC).
About 15% of lung cancers (less than 1 in 5) are small cell; the rest are non-small cell
Small cell lung cancer is called this because when the cancer cells are looked at under a microscope they are very small.
Small cell lung cancer is usually caused by smoking, and it is rare for someone who has never smoked to develop this type of lung cancer. Small cell lung cancer is often fast-growing and can spread quickly.
There are three main types of non-small cell lung cancer. Sometimes it is not possible to tell which type someone has. This is because when the cells are looked at under a microscope, they are not developed enough or the biopsy doesn't contain enough cells to diagnose the different types of NSCLC.
- Squamous cell carcinoma- This develops in the cells that line the airways. This type of lung cancer is often caused by smoking.
- Adenocarcinoma - This is the most common subtype. This develops from the cells that produce mucus in the lining of the airways. This type of cancer is becoming more common.
- Large cell carcinoma -This gets its name from the large, rounded cells that are seen when they are examined under a microscope. It is sometimes known as undifferentiated carcinoma.
This is a cancer of the membrane that covers the surface of the lungs and lines the inside of the chest. It often occurs in people who have been exposed to asbestos.
Mesothelioma is a cancer of the mesothelium. This is a thin lining (membrane) that covers the outer surface of many organs in the body. It also lines the spaces (cavities) within the body, such as the chest and abdominal cavity.
The mesothelium has different names depending on where it is in the body. For example:
- the mesothelium in the chest is called the pleura
- the mesothelium the tummy (abdomen) is called the peritoneum.

In the UK, more than 2,700 people are diagnosed with mesothelioma each year.
The most common cause of mesothelioma is exposure to asbestos. Over 9 out of 10 cases of mesothelioma (90%) are caused by exposure to asbestos fibres. Asbestos is a natural mineral found in many countries.
- The symptoms of pleural mesothelioma may include:
- shortness of breath
- chest pain that feels heavy, dull or aching
- a high temperature (fever) and heavy sweating at night
- extreme tiredness (fatigue)
- weight loss
- loss of appetite
- a cough that does not go away.
Investigation normally takes place in the pleural clinic
Neuroendocrine Tumours (NENs) is an umbrella term used to cover a group of cancers that start in neuroendocrine cells. These cancers may also be referred to as NETs, NECs, or even Carcinoids. NENs occur when neuroendocrine cells stop working normally and start to grow or behave abnormally.
There are 2 key types of NEN:
- NETs (neuroendocrine tumours) are called ‘well-differentiated’ and tend to have a slow to moderate growth pattern.
- NECs (neuroendocrine carcinomas) – are called ‘poorly differentiated’ and tend to grow rapidly.
Neuroendocrine cells are present throughout the respiratory tract (lungs) as part of the normal anatomy. Lung NENs account for up to 20% of all lung cancers.
To date 5 types of Lung NET have been identified:
- Typical Carcinoid (TC) low grade neuroendocrine tumour (NET)
- Atypical Carcinoid (AC) mid-grade neuroendocrine tumour (NET)
- Small cell neuroendocrine carcinoma (NEC)
- Large cell neuroendocrine carcinoma (NEC)
- MiNEN or mixed cell carcinoma (MiNEN) – where Neuroendocrine cells occur within the same tumour as another form of cancer.
Investigations: You will likely have a CT Scan, PET scan and a biopsy either EBUS or CTGBX.
How is Neuroendocrine Cancer Treated?
For all patients, there are many things to consider in planning treatments. Your treatment will be personalised to you and the type of Neuroendocrine Cancer you have. Even if you have a diagnosis that sounds the same as another patient, your treatment and follow up plan may be different. You will be referred to the NET MDT in Birmingham, that specialise in the management of these tumours.
The key aim of treatment should be to help you have the best possible care and quality of life, by ensuring access to appropriate treatment, management of symptoms and addressing what’s most important to you.
One or more of the approaches below may be suggested:
- Removal of all or part of your NEN
- Control of your disease, by slowing or stopping the growth
- Palliation, or easing of your symptoms.
Neuroendocrine Cancer - Neuroendocrine Cancer UK Carcinoid syndrome | Macmillan Cancer Support

- Thymomas and thymic carcinomas are rare cancers that form on a gland called your thymus.
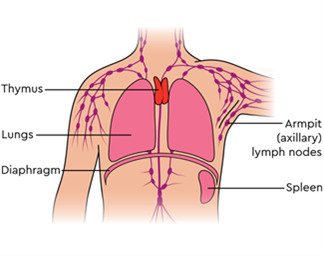
- The thymus gland is in the chest, between the lungs and behind the breastbone or sternum. It is just in front of and above the heart.
- The thymus makes white blood cells called T lymphocytes. These are also called T cells. These are an important part of the body's immune system, which helps to fight infection.
- The thymus gland grows to its largest size during childhood and makes all the T cells we need before we become teenagers. After this, it gradually gets smaller, becomes less active and is replaced by fatty tissue.
- Usually, enlargement of the Thymus gland does not cause any symptoms
- When symptoms are present, they may include chest pressure or pain, cough, shortness of breath, trouble swallowing.
- Very rarely, they can cause a medical condition- Myasthenia Gravis https://www.nhs.uk/conditions/myasthenia-gravis/
- You will normally be asked to have imaging investigations ahead of any treatment. These can include:
- PET/CT scan further information
- MRI Chest further information
Treatment is normally by surgical removal of the whole Thymus gland
For information around the staging of your lung cancer please visit TNM staging for lung cancer
When you are told you have a nodule in your lungs it can be confusing, and you may have questions. This webpage has been produced to help explain what it means to have a lung nodule, and to reassure you about what to expect.
What does ‘lung nodule’ mean?
The phrase ‘lung nodule’ describes a small, denser area of the lung which appears as a round spot on the image. Finding a nodule on a chest X-ray or CT scan is common.
Common Features:
- Often small, measuring less than 30 millimeters
- Don’t have any symptoms, and
- Do not affect the function of the lungs or interfere with breathing.
- Sometimes a lung nodule is also called a ‘pulmonary’ nodule and the two phrases mean the same thing.
How common is it to have a lung nodule?
Up to 35 percent of people who have a CT scan which includes their lungs will have a nodule found.
Sometimes it is possible to find more than one nodule in your lungs. This is not necessarily more serious than having a single nodule.
What might have caused my lung nodule?
The nodule can be due to lots of different causes. These can include:
- a small area of infection
- scarring
- normal glands within the lung
- nodules are common in people who have had previous TB
- In a small number of cases, they can be the first signs of an early cancer in the lung. If this is the case, finding them early makes them much more treatable.
How will my lung nodule be followed up?
It is not always possible to tell what a nodule represents on the very first scan. In these cases, we may offer you one or more further scans to see if the nodule changes or stays the same over a period of time.
Most lung nodules stay the same size, get smaller, or even disappear. If the nodule has not increased in size over several scans, no more follow-up is required. The majority of lung nodules do not change.
The process of repeated scans and reviewing results is sometimes called ‘nodule surveillance’ or ‘active monitoring’.
Not all lung nodules require more follow-up. We use national guidelines which have been written using evidence from clinical studies of thousands of people’s scans and their outcomes. These guidelines and the features described help us to decide what to do next with each sort of nodule, and pick out any that might need follow up.
Your doctor or specialist nurse will talk to you about your individual risk and you can always ask any questions if you have them.
Support for you and your family
If you have a scan which shows a lung nodule, a multi-disciplinary team (MDT) work together to look after you. The team might include consultant respiratory physicians, specialist trainee doctors, a consultant radiologist and a specialist nurse.
Your appointments will normally be with a respiratory physician or specialist nurse to discuss results of your scans and next plans.
These might be face to face, over the telephone, via video clinics or through letters.
If you do have worries or anxieties, especially between appointments, it’s important to talk to them about this.
Summary
Lung nodules are very common findings, and your team are there to support and work with you and to answer any questions you have. If you’d like to find out more have a look at the leaflets below.
Lung Health Checks Lung nodules leaflet - Lung nodules
Frequently asked questions leaflet - FAQ
Lung nodule video - www.youtube.com/watch?v=J6oyYwqTjPo